Cholesterol (Part II) - The Case For Discussion
In the text published last week, I began by recalling a very common belief: the consumption of foods rich in cholesterol is closely linked to an increased risk of developing cardiovascular diseases.
I mentioned that this assumption would only be partially correct and started by pointing out the fact that cholesterol and phospholipids account for only about 5% of lipids obtained from food, with the remaining 95% referring to triglycerides. (link)
However, cholesterol and triglycerides are the main "cargo" transported by lipoproteins, and among these, LDLs are the lipoproteins with the highest atherogenic potential. As we saw in the previous text, the higher the number of LDL particles, the greater the possibility of atherosclerosis development.
Thus, how can we shape our diet to decrease the number of LDL particles and not promote the emergence of atherosclerotic plaques in our vessels?
Before answering this question, it is essential to understand how atherosclerosis develops. In summary:
1. As the number of atherogenic particles in our bloodstream increases (particles containing ApoB, mainly LDLs - as mentioned in the previous text), the probability of these entering the subendothelial space of our vessels increases;
2. In these locations, an inflammatory response is activated, promoting the adhesion of LDL and its content to this space;
3. With the progression of the inflammatory response, a greater number of particles enter, contributing, through this fixation and inflammation itself, to the destruction of the arterial wall;
4. Thus, the arterial lumen decreases, eventually forming fibrous caps that can lead to the creation of atherosclerotic plaques (with local blood clots, for example) which, when dislodged, can become lodged in other locations where they can obstruct blood flow, leading to acute myocardial infarction, for example.
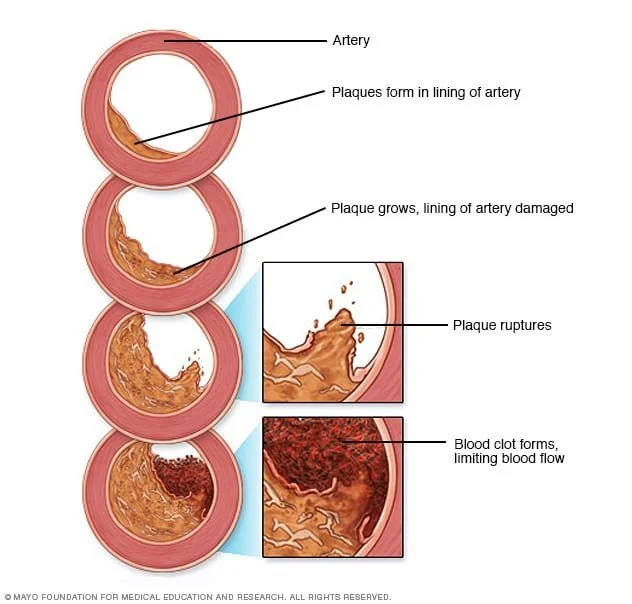
Image 1 - Source: Mayo Foundation
Since the second half of the 20th century, the discussion around fat consumption has sparked extremely heated debates, creating barricades with people adopting extreme positions. It began with a declared war on cholesterol, because it was believed that its consumption through diet should be avoided as much as possible, and major campaigns were launched. Even during this initial period, some studies began to partially question this causal relationship. More recently, studies and books have been published referring to the fact that dietary fats have no negative impact on our health and, on the contrary, should be a significant part of a healthy diet. In the midst of all this, it is easy to become confused and unsure of what we should ultimately eat.
Image 2 - Source: Time Magazine
However, if the various sides of this (possibly endless) discussion almost constantly disagree and exchange contradictory arguments, one thing cannot be denied by any side:
In recent years, even the most responsible and recognized global scientific associations have been adopting an increasingly tolerant attitude towards the consumption of healthy lipid-rich foods. (link)
With this text, my goal is not to advocate for one side or the other, but to try to show, through the best-known facts about cholesterol metabolism and the development of atherosclerosis, the potential that some forms of nutritional intervention can have; trying to contribute, in this way, to a discussion that should be productive and not dogmatic.
Taking into account the mechanisms and causal relationships that I explained earlier, in order to decrease our cardiovascular risk, we should adjust our diet according to these two levels of intervention:
1. Decreasing the number of LDL particles in circulation
2. Reducing the development of atheromatous plaques
Decreasing the number of LDL particles in circulation
When I mentioned that cholesterol and phospholipids account for about 5% of the lipids we ingest, I did not say that cholesterol alone could be about 3% of the total of these lipids. From this amount, it is important to note that only a minority will be absorbed through our intestines. The reason is that the vast majority of dietary cholesterol is esterified, which (due to its size, in this state) prevents it from being absorbed. (link)
Thus, the overwhelming majority of cholesterol present in our LDL does not come from the diet; however, these lipoproteins contain another particle that represents 95% of the lipids we ingest: triglycerides. Many foods rich in cholesterol are also rich in triglycerides, such as saturated and trans fats. In this field, in particular, they should be avoided due to their rich triglyceride content and not their cholesterol. It is important that this message reaches both professionals and users.
Carbohydrates should also enter this equation due to the fact that, through a process called de novo lipogenesis, when we consume this type of nutrient in excess, there is a phenomenon of converting carbohydrates into fatty acids, which are later stored as triglycerides. Later, these triglycerides can be used as an energy source through a process called beta-oxidation. However, whenever these triglycerides need to pass through circulation, there will be an increase in the number of LDL particles to transport them. (link)
It is also described that in people with insulin resistance, or even fully established Diabetes mellitus (sometimes due to excessive carbohydrate consumption), there is often an increase in the triglyceride/cholesterol ratio within their LDL; resulting in an increase in the total number of particles (LDL-p) and a decrease in the amount of cholesterol in them (LDL-c). (link)
Up to this point, the relationship between the consumption of different types of foods and their cardiovascular risk is practically linear: excessive consumption of saturated or trans fats and carbohydrates can lead to an increase in circulating triglyceride levels, which, by leading to an increase in the number of LDL particles in circulation, raises the risk of atherosclerosis. Despite this, what we eat also influences the development of this pathology in a more indirect way, related to the main characteristic of atherosclerotic disease: it is an inflammatory process.
Reducing the development of atheromatous plaques
When intervening at this level, our dietary goal must be only one: to reduce its inflammatory potential.
Diets rich in saturated/trans fats can cause disturbances in the intestinal wall. This may promote the translocation of bacterial products into the circulation and initiate a pro-inflammatory state due to endotoxins' action. The most important of these is lipopolysaccharide, which may lead the development of inflammatory responses in the host, particularly at the cardiovascular level: atherosclerosis. (link)
Lipopolysaccharide can also increase circulating triglycerides by increasing hepatic synthesis of VLDL (also atherogenic) and decreasing its destruction. (link)
This inflammatory potential of the diet gains special importance when fat or carbohydrate sources are highly processed foods or come from animals that have been artificially fed and subjected to supplementation, as all of this greatly increases their inflammatory potential.
It will be important, in addition to not damaging the intestinal wall, to try to promote its health, through hydration and the intake of fiber-rich foods; and in cases of intolerances, to respect them and avoid sources of nutrients that the body cannot metabolize effective.
We also need to keep in mind that insulin resistance and hypertension are individual and essential promoters for the development of atherosclerosis. Therefore, dietary measures should always take these factors into account as well.
I hope the last paragraphs of this text have showed that the discussion about diet as a preventive measure for atherosclerosis should be seen from various angles. While there is room to discuss some of the potential harms of excessive consumption of saturated and trans fats in this field, it is important to note that this is much more related to the likely increase in circulating triglycerides and not cholesterol. At the same time, triglycerides can also see their levels increased through excessive carbohydrate consumption. Thus, there will be a greater potential for atherosclerosis through the increase in circulating LDL.
But also, since these nutrients contribute to the development of insulin resistance and hypertension, the development of the vascular pathology in question can also be promoted through this pathway.
In addition to being careful with the quantities of these nutrients in our diet, it will always be necessary to pay great attention to their quality, in order to promote inflammation as little as possible, which, having the intestine as a crucial starting point, should also make us consider adopting extra measures to promote the health of this organ, particularly regarding its microbiota, through the consumption of foods that stimulate it positively.